Blog Posts
Survey of Primary Care Physicians and Health Plan Execturives Seems to Suggest Differing Views of the Present and Future of Healthcare
Results from a recent survey sponsored by Quest Diagnostics and Inovalon (Progress on the Path to Value-Based Care, 2017) show the differing views primary care physicians and health care executives have of the current and future healthcare landscape. The survey, seemingly the second in two successive years, surveyed 302 primary care physicians in private practice and 150 director-level health plan executives.
Of note were the discordant views regarding the usefulness of information technologies in advancing value-based care, with health plan executives being more positive about their overall usefulness than their primary care counterparts (53% versus 44%, respectively.) This wasn’t surprising given the fact that most physicians aren’t likely aware of how gathering aggregate patient data can lead to insights that many health plan executives are already aware of from their work with accountable care organizations.
Perhaps more interesting (in my view) was the finding that 82% of the whole group surveyed said they believed that the transition to valve-based care would continue, but it appeared from the breakdown of physicians by years in practice (over 21 years versus 20 years or less) that those who have been around longer were not seeing the changes as readily as those who were in practice less than 20 years; 16% versus 31%, respectively.
The survey did not theorize why there was this difference. Perhaps those in practice longer are not as “tuned in” to the changes on the horizon. Perhaps there was a difference in the percentage of practices adopting EHRs based upon years in practice. One can certainly hope that this difference in awareness is not a difference in belief regarding the inevitability that healthcare is moving solidly toward accountability in outcomes and cost, whether we are ready or not.
Of note were the discordant views regarding the usefulness of information technologies in advancing value-based care, with health plan executives being more positive about their overall usefulness than their primary care counterparts (53% versus 44%, respectively.) This wasn’t surprising given the fact that most physicians aren’t likely aware of how gathering aggregate patient data can lead to insights that many health plan executives are already aware of from their work with accountable care organizations.
Perhaps more interesting (in my view) was the finding that 82% of the whole group surveyed said they believed that the transition to valve-based care would continue, but it appeared from the breakdown of physicians by years in practice (over 21 years versus 20 years or less) that those who have been around longer were not seeing the changes as readily as those who were in practice less than 20 years; 16% versus 31%, respectively.
The survey did not theorize why there was this difference. Perhaps those in practice longer are not as “tuned in” to the changes on the horizon. Perhaps there was a difference in the percentage of practices adopting EHRs based upon years in practice. One can certainly hope that this difference in awareness is not a difference in belief regarding the inevitability that healthcare is moving solidly toward accountability in outcomes and cost, whether we are ready or not.
____________________________________________________________________________
The Bipolar Bridge
I was reviewing an online CME presentation through Medscape (Managing Patients with Bipolar Disorder and Mixed Features CME
Trisha Suppes, MD; Terence A. Ketter, MD; Susan L. McElroy, MD), and, as part of the presentation, a slide was shown to point out the "newer" conceptualization of the Bipolar diagnosis in DSM-5. It is about time.
For years the concept of mood disorder (and many disorders presented in the Diagnostic and Statistical Manual from I to IV) were thought of as existing in distinct and separate categories. Anyone who treats people with these conditions long enough knows that individuals rarely present with distinct, categorical diagnoses. They usually present with clusters of symptoms, overlaps of comorbidities, and a general "mashup" of distresses that need teased from one another before treatment can take hold. The newer framework of conceptualizing and describing this condition is a welcomed addition.
Trisha Suppes, MD; Terence A. Ketter, MD; Susan L. McElroy, MD), and, as part of the presentation, a slide was shown to point out the "newer" conceptualization of the Bipolar diagnosis in DSM-5. It is about time.
For years the concept of mood disorder (and many disorders presented in the Diagnostic and Statistical Manual from I to IV) were thought of as existing in distinct and separate categories. Anyone who treats people with these conditions long enough knows that individuals rarely present with distinct, categorical diagnoses. They usually present with clusters of symptoms, overlaps of comorbidities, and a general "mashup" of distresses that need teased from one another before treatment can take hold. The newer framework of conceptualizing and describing this condition is a welcomed addition.
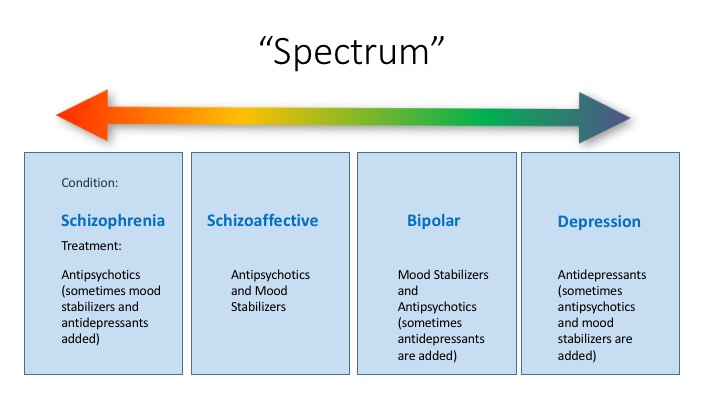
The above is a slide from the presentation listed above noting how Bipolar Disorder previously was described in either "Manic, Mixed, or Depressive" episodic terms. In DSM-5, the condition becomes more of a spectrum in presentation where the previous "mixed" episode can have features that make it more "manic" or more "depressive." When I saw this slide that Dr. Suppes produced, it reminded me of some presentations and readings from the past where the field was increasingly seeing the major disorders as less categorical and more on a spectrum. For instance, it has become clearer over the years that genetic, comorbidity, outcome, and structural data is increasingly supporting the concept that Schizoaffective Disorder lies somewhere in between Bipolar Disorder and Schizophrenia in all of its forms (Baron, et. al, Acta psychiat. stand. (1982) 65, 253-262. Laursen et. al, J Clin Psychiatry 2009;70(10):1432-1438, Abrams et. al., Neuropsychiatric Disease and Treatment 2008: 4(6) 1089-1109). It is "middle" in terms of severity of condition, longitudinal outcome, and perhaps treatment resistance. Therefore, it would not be unusual to envision a conceptualization of the aforementioned disorders in the following fashionThis also might explain why some individuals with Schizophrenia seem to be helped by the addition of traditional mood stabilizing agents and why individuals with Bipolar Disorder sometimes need an antidepressant in their regimen, despite the fact that all of the evidence we have at our disposal seems to suggest that antidepressants and bipolarity makes things worse. It may be best to think of all of these conditions as simply one continuum.

Opening Old Wounds. The Paxil® Story
The British Medical Journal (BMJ) recently published the results of a reanalysis of an original study published in the Journal of the American Academy of Child & Adolescent Psychiatry (JAACAP) in 2001. The JAACP is the foundational journal of child and adolescent psychiatrists, often serving as the first resource in guiding psychiatric treatment for our patients.
The BMJ’s publication was the first of its kind, a reanalysis of data from a previously published study, and subsequently publishing those results. The results of the study not only demonstrated (again) that the original data did not demonstrate efficacy of Paxil®, but also suggested additionally that data was suppressed purposefully, that ratings of the original patient level data were “under interpreted,” and data points that would have demonstrated efficacy were kept from the publication. All of this seemed to suggest that the original authors were deliberately trying to hide facts not in the medication’s favor. This came about through the RIAT initiative which stands for “Restoring Invisible and Abandoned Trials.”
The original publication (Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in the treatment of adolescent major depression: a randomized, controlled trial. J Am Acad Child Adolesc Psychiatry 2001;40:762-72) proclaimed that Paroxetine (Paxil®) was “generally well tolerated and effective.” Note, the publication was initially rejected by JAMA, but accepted by the JAACAP. The publication guided those of us on the frontline to use Paxil in an effort to combat Major Depression in the pediatric population. This has been a difficult entity to treat over the years, particularly because many of the agents available at the time found effective for adults were found ineffective for children (tricyclic antidepressants, for example). A co-author of that publication, Karen Wagner, MD, reportedly promoted the agent at a Galaxo Smith Klein (GSK) sales force event in 1999, saying, “We can say that paroxetine has both efficacy and safety data for treating depression in adolescents.” The newsletter apparently stated that the study demonstrating the success of their medication would be published in a peer reviewed journal. Unfortunately, that assessment, as it turns out, was completely wrong.
Data from Europe showing a signal that suicidal thinking was increased in adolescent patients taking paroxetine resulted in the study being terminated early and, in the US at least, the medication class receiving a “black box” warning about an increase in suicidal thinking in children, adolescents and eventually young adults. The FDA obtained data from GSK and the study published in 2001 and determined that data did not prove efficacy. The US Department of Justice raised criminal charges against GSK for marking off-label and was fined a record three billion dollars.
The BMJ republication noted that not only did the paroxetine not demonstrated efficacy in the reanalysis, there were also 12 cases of suicidality where the original publication found 5 and, as noted in an article published by Medscape (New Analysis of Paxil Data: Were Adverse Events Downplayed? | Medpage Today, Fiore, K., http://www.medpagetoday.com/Psychiatry/GeneralPsychiatry/53583) ""There were several of, what looks like to the impartial observer, deliberate attempts to play down the adverse effect profile," Jureidini said during a press call with editors from the BMJ, where the study was published. 'We can't be definite about that, but that's what it looks like.’"
By the time the controversy about Paxil’s® efficacy came into question, many child psychiatrists like myself had moved on. The agent was often simply too sedating, causing too much weight gain, and problematic with withdrawal symptoms when missing doses that we had set it aside. However, this reawakening of the controversy with the BMJ’s publication brings another chill to those of us who have to trust these sources when it comes to making decisions about our patient’s lives. Perhaps the most chilling of all is the fact that despite all of this information being presented, the lawsuit, the republication, and calls for retraction, the journal of our specialty society refuses to retract the original paper. In a letter sent to all of its membership, they indicated little responsibility for the information and passed it along to the authors of the study. One wonders if the fact that Dr. Karen Wagner, one of the original authors and paid educator for GSK being president-elect of the AACAP has anything to do with it.
Other References: Le Noury J, et al "Restoring Study 329: Efficacy and harms of paroxetine and imipramine in the treatment of major depression in adolescence" BMJ 2015; DOI: 10.1136/bmj.h4320
Doshi P "No correction, no retraction, no apology, no comment: Paroxetine trial reanalysis raises questions about institutional responsibility" BMJ 2015; DOI:10.1136/bmj.h4629
The BMJ’s publication was the first of its kind, a reanalysis of data from a previously published study, and subsequently publishing those results. The results of the study not only demonstrated (again) that the original data did not demonstrate efficacy of Paxil®, but also suggested additionally that data was suppressed purposefully, that ratings of the original patient level data were “under interpreted,” and data points that would have demonstrated efficacy were kept from the publication. All of this seemed to suggest that the original authors were deliberately trying to hide facts not in the medication’s favor. This came about through the RIAT initiative which stands for “Restoring Invisible and Abandoned Trials.”
The original publication (Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in the treatment of adolescent major depression: a randomized, controlled trial. J Am Acad Child Adolesc Psychiatry 2001;40:762-72) proclaimed that Paroxetine (Paxil®) was “generally well tolerated and effective.” Note, the publication was initially rejected by JAMA, but accepted by the JAACAP. The publication guided those of us on the frontline to use Paxil in an effort to combat Major Depression in the pediatric population. This has been a difficult entity to treat over the years, particularly because many of the agents available at the time found effective for adults were found ineffective for children (tricyclic antidepressants, for example). A co-author of that publication, Karen Wagner, MD, reportedly promoted the agent at a Galaxo Smith Klein (GSK) sales force event in 1999, saying, “We can say that paroxetine has both efficacy and safety data for treating depression in adolescents.” The newsletter apparently stated that the study demonstrating the success of their medication would be published in a peer reviewed journal. Unfortunately, that assessment, as it turns out, was completely wrong.
Data from Europe showing a signal that suicidal thinking was increased in adolescent patients taking paroxetine resulted in the study being terminated early and, in the US at least, the medication class receiving a “black box” warning about an increase in suicidal thinking in children, adolescents and eventually young adults. The FDA obtained data from GSK and the study published in 2001 and determined that data did not prove efficacy. The US Department of Justice raised criminal charges against GSK for marking off-label and was fined a record three billion dollars.
The BMJ republication noted that not only did the paroxetine not demonstrated efficacy in the reanalysis, there were also 12 cases of suicidality where the original publication found 5 and, as noted in an article published by Medscape (New Analysis of Paxil Data: Were Adverse Events Downplayed? | Medpage Today, Fiore, K., http://www.medpagetoday.com/Psychiatry/GeneralPsychiatry/53583) ""There were several of, what looks like to the impartial observer, deliberate attempts to play down the adverse effect profile," Jureidini said during a press call with editors from the BMJ, where the study was published. 'We can't be definite about that, but that's what it looks like.’"
By the time the controversy about Paxil’s® efficacy came into question, many child psychiatrists like myself had moved on. The agent was often simply too sedating, causing too much weight gain, and problematic with withdrawal symptoms when missing doses that we had set it aside. However, this reawakening of the controversy with the BMJ’s publication brings another chill to those of us who have to trust these sources when it comes to making decisions about our patient’s lives. Perhaps the most chilling of all is the fact that despite all of this information being presented, the lawsuit, the republication, and calls for retraction, the journal of our specialty society refuses to retract the original paper. In a letter sent to all of its membership, they indicated little responsibility for the information and passed it along to the authors of the study. One wonders if the fact that Dr. Karen Wagner, one of the original authors and paid educator for GSK being president-elect of the AACAP has anything to do with it.
Other References: Le Noury J, et al "Restoring Study 329: Efficacy and harms of paroxetine and imipramine in the treatment of major depression in adolescence" BMJ 2015; DOI: 10.1136/bmj.h4320
Doshi P "No correction, no retraction, no apology, no comment: Paroxetine trial reanalysis raises questions about institutional responsibility" BMJ 2015; DOI:10.1136/bmj.h4629